#############






Effect of Different Milk Diet on the Level of Fecal Calprotectin in Very Preterm Infants
 Simonetta Costa*,
Simonetta Costa*,  Maria Letizia Patti,
Maria Letizia Patti,  Alessandro Perri,
Alessandro Perri,  Carmen Cocca,
Carmen Cocca,  Giovanni Pinna,
Giovanni Pinna,  Chiara Tirone,
Chiara Tirone,  Milena Tana,
Milena Tana,  Alessandra Lio and
Alessandra Lio and  Giovanni Vento
Giovanni Vento- Department of Woman and Child Health and Public Health, Child Health Area, Fondazione Policlinico Universitario A. Gemelli, IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
Objective: To evaluate the course of fecal calprotectin (FC) in very preterm infants over the first 15 days of life in relation to the type of milk diet.
Methods: This study was part of a randomized controlled trial comparing two different ways of integrating the own mother's milk (OMM) for the evaluation of feeding tolerance in very preterm infants. In infants with gestational age of ≤ 32 weeks randomized to receive preterm formula (PF group) or pasteurized donor human milk (PDHM group) as a supplement to the OMM insufficient or unavailable, FC level was planned to be measured at the first meconium passage and at days 8 and 15 of life (T0, T1, and T2, respectively).
Results: FC data were available for all the 70 infants randomized, 35 in the PF group, and 35 in the PDHM group. The mean FC levels were similar in the two study groups at T0 and T1, whereas they were significantly higher in the PF group than the PDHM group at T2. FC values decreased over the first week of life in both groups and significantly increased over the second week of life only in the PF group.
Conclusions: Our study demonstrates a significant increase in FC levels when PF is used as a supplement to the OMM compared to the use of PDHM. Further studies are needed to establish if the higher FC levels in infants receiving PF are the expression of a normal immunological maturation rather than an initial inflammatory process.
Introduction
Calprotectin is a 36.4-KDa calcium and zinc-binding protein that constitutes the main component of cytosolic protein of neutrophils, monocytes, and macrophages. Calprotectin was shown to have bactericidal and fungicidal properties, and it may be involved in the regulation of inflammation (1, 2). Calprotectin is found in various body fluids in proportion to the degree of inflammation, but its concentration in the stool is ~6 times that of the plasma: this is the reason why the measurement of fecal calprotectin (FC) would likely be a sensitive and specific marker of gastrointestinal inflammation. The level of FC can be proportional to the quantity of neutrophils migrating through the gastrointestinal mucosa (3, 4).
In adults and children, FC is greatly used as a noninvasive marker for the diagnosis of inflammatory bowel disease and may serve as an important clinic test in order to evaluate the inflammatory state of the whole intestinal tract (5, 6). The reference value given for healthy adults and children older than 4 years of age is 50 μg/g of feces (7).
The current evidence suggests that FC is elevated in newborn infants suffering from necrotizing enterocolitis, but its significance as an early screening marker remains unknown. The reported sensitivity and specificity of the test remain unidentified, as there is a lack of consensus regarding the implementation of specific cutoff values (8).
Conflicting results have also been reported on the effect of the kind of feeding on the level of FC in infants. Some studies have shown higher FC in exclusively breastfed infants when compared to mixed- or formula-fed ones, and some have shown no difference (9–20).
The aim of this study was to evaluate the time course of FC in very preterm infants over the first 15 days of life in relation to the different kind of milk diet.
Materials and Methods
This study was part of a single-center, randomized, non-inferiority trial comparing two different ways of integrating the own mother's milk (OMM) over the first 2 weeks of life for the evaluation of feeding tolerance in very preterm infants (21). Briefly, the clinical trial planned that infants with gestational age (GA) of ≤ 32 weeks, without congenital malformations, connatal infections, or abnormal antenatal Doppler flow velocimetry, and for whom OMM was unavailable or insufficient to satisfy the planned enteral intakes, were randomized to receive pasteurized donor human milk (PDHM) or preterm formula (PF) as a supplement to the OMM. The PF diet consisted of 3.5 g of protein/100 Kcal formula (Plasmon PreZero, Plasmon, Italy). Donor human milk came from mothers who prematurely delivered and pasteurized within 24 h of collection by the Holder method (+ 62.5°C for 30 min). Minimal enteral feeding was initiated within the first 48 h of life and was continued at 20 ml/kg/day for up to 5 days. Subsequently, enteral nutrition volume was increased by 20 ml/kg/day. The parenteral nutrition (PN) was started soon after birth in all infants with a birth weight (BW) of <1,250 g and in infants with BW of <1,500 g requiring invasive ventilation. The PN was stopped when enteral intake was >125 ml/kg/day.
FC level was measured at the first meconium passage and at days 8 and 15 of life (T0, T1, and T2, respectively).
Stool samples were taken from the infants' diapers with sterile plastic spoons and put in sterile plastic screw-cap tubes. The samples were then frozen at −80°C until analysis. One hundred milligrams of stool were weighed, placed in a 15-ml conical tube, and agitated with a wooden stirrer. An extraction buffer was added, the sample vortexed to form a fine slurry, and then placed on a shaker for 25 min. One milliliter was removed and centrifuged at 10,000 g for 20 min. The supernatant was removed for analysis by ELISA (Eurospital, Trieste, Italy). The FC was expressed as μg/g of stool. Every assay included a standard curve and quality controls, all samples were done in duplicate, and the intra-assay coefficients of variation were <10%.
All parameters were checked for normal distribution using the Shapiro–Wilk test. Differences between the two groups were investigated using paired Student's t-test for normally distributed data or Wilcoxon signed-rank test otherwise. Chi-square test was used to compare categorical data. Data are presented as mean ± standard deviation (SD) or median–interquartile range. A p-value of <0.05 is considered to indicate statistical significance. Statistical analysis was performed using XLSTAT version 2014.5.03.
The institutional review boards approved the study, and written informed consent was obtained from the parents of all subjects before enrollment.
Results
FC data were available for all the 70 preterm infants randomized in the original trial, 35 in the PF group and 35 in the PDHM group. Demographic and clinical data were well balanced between the two study groups, as detailed in Table 1.
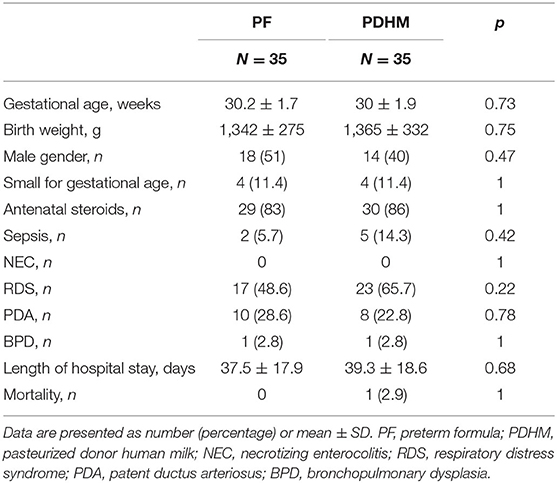
Table 1. Demographic and clinical data.
There was no difference in the maximum weight loss, but infants in the PF group regained birth weight 2 days earlier than infants in the PDHM group. No difference was observed in the duration of fasting, minimal enteral feeding, and parenteral nutrition. Time to reach full enteral feeding of 150 ml/kg/day of milk was similar in the two study groups. Infants in both groups received a similar total intravenous and enteral fluid intake, such as a similar amount of OMM, whereas the amounts of PF and PDHM were significantly different between groups, as expected (Table 2).
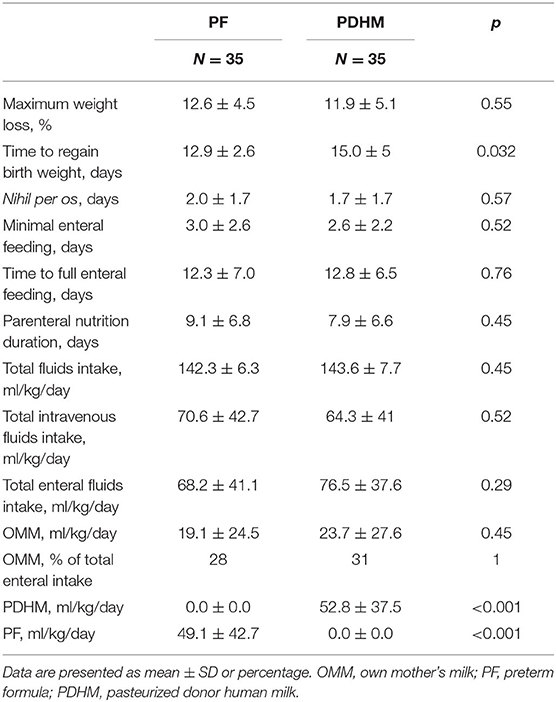
Table 2. Nutritional data and milk intakes over the first 15 days of life.
The mean FC levels were similar in the two study groups at T0 and T1, whereas they were significantly higher in the PF group than the PDHM at time 2 (Table 3).
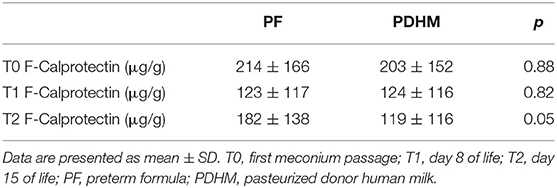
Table 3. Fecal calprotectin levels over the study period.
FC values decreased over the first week of life in both groups and increased in a significant manner in the second week of life only in the PF group (Figure 1).
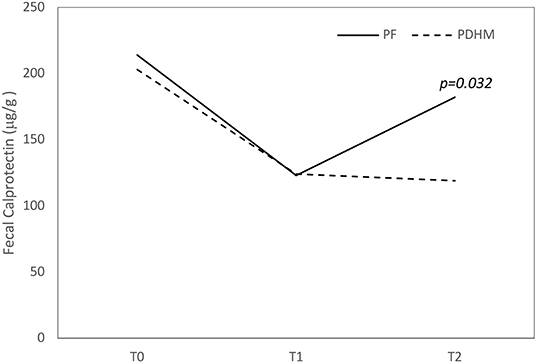
Figure 1. Trend of fecal calprotectin values over the first 15 days of life. The figure shows that fecal calprotectin concentration decreased over the first week of life in both groups and increased at 15 days only in the PF feed group. PF, preterm formula; PDHM, pasteurized donor human milk.
Discussion
In this study, we observed significantly higher FC levels at 15 days of life in very preterm infants who received PF as integration to OMM compared to those infants who received PDHM.
Previous studies reported conflicting results on the effect of feeding on the FC levels in infants since some authors observed higher FC levels in breastfed infants compared to mixed- or formula-fed ones (9–13), while others authors found no difference in the FC levels of infants fed breast milk vs. formula (14–20).
It is a challenge to explain why FC levels are higher in breastfed infants than formula-fed ones since FC is an index of bowel inflammation. On the contrary, it is evident that human milk contains several anti-inflammatory bioactive components that promote intestinal growth and maturation and reduce intestinal permeability more than formulas (22–25). It has been hypothesized that higher FC in breastfed neonates could be consistent with the promotion of maturation of the intestinal mucosa. High FC in the gut, induced by human milk, could provide a protective effect through its bactericidal and fungicidal properties and could contribute to modulation of the intestinal microflora (10, 11, 13).
This hypothesis seems to do not support our results as we found higher FC levels in the PF group compared to the PDHM group. We supposed that the significantly higher FC values in formula-fed infants at the 15th day of life could be explained with a subclinical inflammation of the bowel induced by PF.
It has been reported that preterm infants with feeding intolerance have statistically significant elevated levels of FC than those without feeding intolerance (26, 27) and that the FC levels decrease in a significant manner when PF-fed infants with feeding intolerance were shifted to receive amino acid-based formula (27). In our original trial, the infants who received PF as integration to OMM had a similar feeding tolerance than those who integrated their OMM with PDHM, since the time to achieve the full enteral feeding was the same for both groups (21), so we cannot attribute the higher FC levels in preterm infants receiving PF to the feeding intolerance.
A significant positive correlation has also been observed between the amount of volume of enteral feeding and FC levels (17, 28), suggesting that exposure to the increasing luminal dietary antigens might induce a state of physiological subclinical intestinal inflammation and then an increase in the calprotectin in the gut lumen. In our study, infants in both groups received the same mean enteral fluid intake, but FC increased significantly at 15 days of life only in the PF group.
It is almost evident that the type of milk diet influences the diversity of the gut microbiota in infants. The greatest microbial richness has been found in infants exclusively fed OMM (29). Cong et al. (30) found a more favorable microbial community in infants receiving exclusively OMM and a significantly lower diversity and a different microbial community in infants receiving PHDM and PF compared to infants receiving OMM. In particular, these authors found that infants receiving OMM had the highest abundance of Clostridiales, Lactobacillales, and Bacillales and the lowest abundance of Enterobacteriales. The groups of infants receiving OMM+PHDM as well as those infants receiving OMM+PF also had higher abundance of Clostridiales, Lactobacillales, Bacillales, and Bacteroidales compared to the groups of infants receiving only PHDM or PF or PHDM+PF (30).
The microbiota related to OMM stimulates the normal development of the gut-associated lymphoid tissue, representing the major external driving force in the maturation of the immune system after birth. When the gut microbiota becomes established, neutrophil infiltration into the intestinal mucosa occurs as an integral part of normal bowel development. This physiological inflammatory process would explain why infants who receive breast milk have higher levels of FC. In our study, infants in both groups received a similar amount of OMM, and the variable that can explain the difference in FC levels is attributable to the PF.
In our study, it is difficult to establish if the higher levels of FC found in PF group infants are the expression of a physiological process of intestinal maturation rather than the beginning of a pathological inflammatory process. However, the levels of FC we found were below the lowest reported cutoffs for bowel pathology in preterm infants (31, 32), as well as feeding tolerance was similar in both groups.
Regarding the course of FC over the first 15 days of life, we observed that the FC concentration decreased over the first week of life in both groups and increased at 15 days only in the PF-fed group. The course of FC in PF group infants is consistent with that reported by Zoppelli et al. (33), who found that in preterm infants, the FC levels, initially high in the meconium, dropped, reaching a nadir at approximately 8 days of life and then increased in a GA-dependent manner except in the most premature infants with GA <26 weeks. We could speculate that the failure to increase the FC levels in PDHM group infants might be interpreted as an inappropriate immune response of the bowel as what happens in extremely premature babies probably because the donor human milk, after the pasteurization process, is unable to induce the same maturation process induced by the raw OMM.
Our study has some strengths but also limitations. The strength of our study is that it is part of a randomized controlled trial and therefore there is a good control of all the variables that could influence the levels of FC. A limitation of the study is not having studied the intestinal microbiota which could have given more information about the significance of FC levels in relation to the integration of OMM with PF.
Our study demonstrates a significant increase in FC levels when PF is used as a supplement to the OMM when insufficient or unavailable compared to the use of PDHM.
Further studies are needed to establish whether this increased FC levels is the expression of a normal immunological maturation process rather than an initial inflammatory process related to the use of PF.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Review Board, Department of Woman and Child Health and Public Health, Child Health Area, Fondazione Policlinico Universitario A. Gemelli, IRCCS; Università Cattolica del Sacro Cuore. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
All authors have read and approved the manuscript for submission have made a substantial contribution to the conception, design, gathering of data and a contribution to the writing and intellectual content of the article and acknowledge that they have exercised due care in ensuring the integrity of the work. SC conceived the design of the study, interpreted the data, and revised it critically for intellectual content. MP drafted the article and interpreted the data. AP analyzed the data for the work. CC, GP, CT, MT, and AL acquired the data and researched the scientific literature. All authors revised the article and have given final approval of the version to be published. GV final approved the work to be published.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Effect of Population Lockdown on Pediatric Emergency Room Demands in the Era of COVID-19
 Francesco Valitutti
Francesco ValituttiObjectives: The aim of this study was to assess the impact of the COVID-19 pandemic and population lockdown on pediatric ED consultations.
Methods: A cross-sectional study on pediatric emergency department consultations before and during the current COVID-19 pandemic (March–May 2019 vs. March–May 2020) was performed in two hospitals in the Campania region (Southern Italy) [i.e., Salerno University Hospital (Salerno) and Pediatric Regional Referral Emergency Hub “AORN Santobono-Pausillipon” (Naples)].
Results: 29,368 consecutive ED pediatric patients (13,430 females; mean age ± SD = 5.4 ± 4.7 years) were seen in March–May 2019 and 9,133 (4,494 females; mean age ± SD = 5.9 ± 4.2 years) in March–May 2020. Resuscitation/emergency and urgent care pediatric ED consultations were 1,388 (4.7%, 95% CI 4.5–4.9) in the 2019 trimester, while they were 648 (7.1%, 95% CI 6.6–7.6) in the 2020 trimester (p < 0.01). Mean pediatric ED daily consultations were 326.3 (95% CI 299.9–352.7) in the considered period of 2019 and 101.4 (95%CI 77.9–124.9) in the same period of 2020 (p < 0.001). COVID-19 nasal swabs were performed for 385 children; of those, six resulted positive and four of them were hospitalized.
Conclusions: This work provides a unique snapshot of the pediatric EDs demands in the era of COVID-19. We witnessed a significant reduction of non-urgent health care demands during the pandemic but an increase of more severe urgent cases. The COVID-19 pandemic and the following lockdown unveiled the inappropriateness of the majority of pediatric ED consultations. Nevertheless, the current scenario highlighted the need for appropriate and timely clinical evaluations in the pediatric primary care to tackle late and more severe diagnoses in EDs.
Introduction
Emergency department (ED) patient flow includes roughly 20–25% of pediatric consultations in western countries each day (1). In Italy, ED visits for children are quite often inappropriate, especially where pediatric primary care is well-structured and could be readily available (2). Since ED overcrowding is a multifaceted issue and a public health hazard, it requires committed policy and medical interventions in order to minimize its related risks (3). In fact, overcrowding in ED has been associated with poor hospital outcomes both in adults and children (4, 5); moreover, it is a well-recognized risk factor for infectious disease spreading (6). Interdisciplinary collaborative research and education are therefore still needed to develop and implement new solutions and strategies to both prevent and manage this serious drawback (7).
On February 21, 2020, the first case of coronavirus disease 2019 (COVID-19), also known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2,) was diagnosed in Northern Italy (8), and a few weeks later, on March 11, 2020, the WHO declared officially it as a pandemic (9).
COVID-19 affects mainly adults whose clinical features display severe interstitial hypoxemic pneumonia (10), but children can be infected, spread the virus, and in almost all cases present a much milder disease (11, 12).
At the beginning of the COVID-19 epidemic, hospital-acquired coronavirus infection may have unknowingly fueled the rising epidemic curve (13), while in the following weeks the population lockdown has strongly tackled its spreading and was confirmed as an effective public health intervention (14).
The Italian government formally announced a national lockdown on March 9: this act implied the complete shutdown for schools, universities, public places, and all the shops but supermarkets, grocers, and pharmacies, along with well-defined traveling restrictions.
However, the current epidemic and population lockdown have dramatically changed worldwide the daily scenario in EDs as regards flows, paths, and disease categories of patients in pursuit of health care.
The aim of our cross-sectional study was to highlight the impact of the COVID-19 pandemic on ED consultation appropriateness for children in two hospitals of Southern Italy, comparing retrospective data from the trimesters March–May 2019 and March–May 2020.
Materials and Methods
We retrospectively evaluated our pediatric ED files of two hospitals in the Campania Region (Southern Italy) [i.e., University Hospital “San Giovanni di Dio e Ruggi D'Aragona” (Salerno) and Pediatric Regional Referral Emergency Hub “AORN Santobono-Pausillipon” (Naples)]. Local internal review boards (Approved regional IRB protocol N. 10 on 28/04/2020 meeting) approved the retrospective chart review of electronic anonymized patient data. We compared medical files of trimester March–May 2019 (no COVID-19 pandemic) vs. files of trimester March–May 2020 (during COVID-19).
ED consultations were triaged by specialized nurses according to the Emergency Severity Index version 4 (ESI v.4), which included five items: (1) resuscitation, (2) emergency care, (3) urgent care, (4) less urgent care, and (5) non-urgent care (15). Appropriate ED visits were defined as: (1) ESI v.4 resuscitation, (2) ESI v.4 emergency care, (3) ESI v.4 urgent care, (4) ESI v.4 less urgent care that nevertheless required prompt investigations not available within the primary care, and (5) ESI v.4 non-urgent care that nevertheless required prompt investigations not available within the primary care.
Involvement of emergency medical transport services (EMTS) (i.e., ambulances) was taken into account and considered as another suitable approximation of clinical severity. EMTS appropriateness was defined as the ratio of urgent and emergency EMTS cases over total EMTS cases. Moreover, we looked at possible temporal patterns of ED consultations, primary care referral rates to the ED, numbers of inpatient hospital admissions, and mean inpatient hospital stay during the two considered periods.
Statistical analysis was performed using IBM SPSS Statistics (IBM Corp., Released 2010; IBM SPSS Statistics for Windows, NY, USA). Data are presented as absolute numbers, percentage, means, and standard deviations. Student's t or chi-squared tests were used to compare subgroup data as appropriate. A p < 0.05 was considered significant for all the tests performed.
Results
Patient demographics and triage classification of the two groups are shown in Table 1.
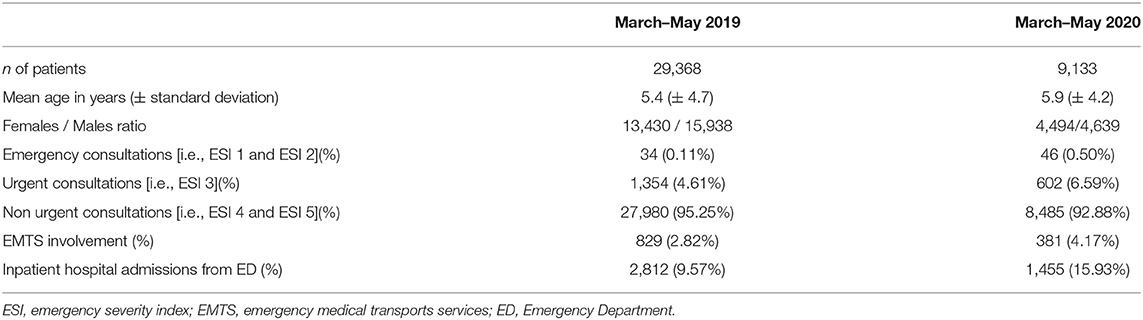
Table 1. Patients demographics in the two considered periods.
Study population included 38,501 children aged from 1 month to 14 years (mean age ± SD: 5.6 ± 4.5 years; 17,924 females) who accessed the EDs of the two hospitals during the two considered periods. Pediatric ED consultations were 29,368 in March–May 2019 and 9,133 in March–May 2020, which accounted for 68.9% reduction in ED utilization for children.
Resuscitation/emergency and urgent care pediatric consultations were 1,388 (4.7%, 95% CI 4.5–4.9) in the 2019 trimester, while they were 648 (7.1%, 95% CI 6.6–7.6) in the 2020 trimester (p < 0.01). Considering only most severe cases, resuscitation/emergency care ED demands for children were 34 (0.11%, 95% CI 0.08–0.14) in 2019 considered period and 46 (0.50%, 95%CI 0.36–0.64) in the same period of 2020 (p < 0.01). Of these, six patients in March–May 2019 and seven patients in March–May 2020 required ICU admission for mechanical ventilation (none of these were COVID-19 positive).
Appropriate consultations were 6,372 (21.7%, 95% CI 21.3–22.1) in 2019 trimester and 2,903 (31.8%, 95% CI 30.9–32.7) in 2020 trimester (p < 0.01).
Primary care referral rates to the EDs was 1.6% (95% CI 1.5–1.7) and 4.6% (95% CI 4.2–5.0) in the 2019 and 2020 trimesters, respectively (p < 0.01).
EMTS was involved for 829 children in March–May 2019 and for 381 children in March–May 2020. EMTS appropriateness was lower in the 3 months of 2019 rather than those of 2020 (12.3 and 18.3%, respectively; p < 0.01).
During night shifts (8 p.m.−8 a.m.), 98.9% (95% CI 98.6–99.2) of the health care requests accounted for non-urgent consultations in March–May 2019, while in March–May 2020 non-urgent consultations were 74.2% (95% CI 72.8–75.6) (p < 0.001).
During weekends (Saturdays and Sundays), 99.1% (95% CI 98.8–99.4) of the ED consultations were represented by non-urgent cases in the 2019 trimester, while in March–May 2020 they were 94.3% (95% CI 92.9–95.7) (p < 0.001).
Mean pediatric ED daily consultations were 326.3 (95% CI 299.9–352.7) in March–May 2019 and 101.4 (95% CI 77.9–124.9) in March–May 2020 (p < 0.001). Considering that the lockdown officially started on March 9, 2020, we saw higher daily consultations in the week from March 1 to March 8 2020 before lockdown (mean: 159.2; 95% CI 136.4–182.0) as compared with the after-lockdown time frame within the same month [i.e., from March 9 to March 31 2020 (mean: 63.3; 95% CI 56.9–69.7) (p < 0.001)].
Mean waiting time for non-urgent consultation was 55.2 min (SD: ± 45.2) in 2019 trimester and 23.1 min (SD: ± 15.7) in March–May 2020 (p < 0.001).
Table 2 summarizes the groups of signs and symptoms prompting ED consultations.
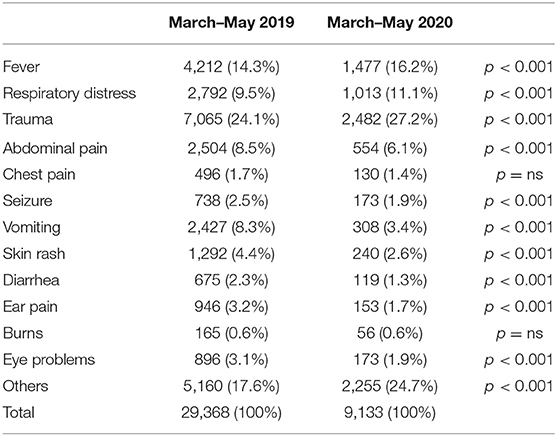
Table 2. Main health problems prompting emergency department consultations.
Higher rates of ED visits were registered in March–May 2020 for fever (16.2 vs. 14.3%, p < 0.001), respiratory distress (11.1 vs. 9.5%, p < 0.001), and traumas (27.2 vs. 24.1%, p < 0.001) compared to those of March–May 2019, albeit absolute numbers in the 2020 trimester were much lower. During the 2020 lockdown, lower rates of ED visits were accounted for abdominal pain (6.1 vs. 8.5%, p < 0.001), seizure (1.9 vs. 2.5%, p < 0.001), vomiting (3.4 vs. 8.3%, p < 0.001), skin rashes (2.6 vs. 4.4%, p < 0.001), diarrhea (1.3 vs. 2.3%, p < 0.001), ear pain (1.7 vs. 3.2%, p < 0.001), and eye problems (1.9 vs. 3.1%, p < 0.001), compared to March–May 2019.
Burns showed a similar rate over the two considered periods (0.6% in the 2019 trimester and 0.6% in the 2020 one, p = ns), but their absolute number was three times before lockdown.
Inpatient hospital admissions following ED consultation were 2,812 in March–May 2019 and 1,455 in March–May 2020, witnessing for a 48.2% reduction during the COVID-19 pandemic. Hospitalization/ED consultation rate was 9.6% in March–May 2019 and 15.9% in March–May 2020 (p < 0.001).
Mean hospital stay duration in the 2019 studied trimester was 5.55 (95% CI 5.07–6.03) days and 5.69 (95% CI: 4.91–6.47) days in March–May 2020 (p = ns).
As regards the number of frailty/chronic disease patients, there were 1,368 ED consultations for children with special needs in March–May 2019 and 1,282 in March–May 2020 (p = ns).
Covid-19 nasal swabs were performed for 385 children; of those, six resulted positive and four of them were hospitalized elsewhere (Pediatric Regional Hub for Infectious Disease); two were quarantined in their house under special medical team follow-up.
Discussion
During the last two decades, both our EDs have usually hosted a vast majority of non-urgent pediatric consultations which would have been better fit for primary care, and our settings do echo other national and international data (16, 17).
In this study, we aimed to assess the impact of the COVID-19 pandemic and population lockdown on pediatric ED consultations and appropriateness analysis. We saw a significant reduction of non-urgent health care demands during the pandemic, most of all after the lockdown had been announced by the Italian government on March 9, 2020. Several factors might explain this finding. First of all, it should be acknowledged that COVID-19 becomes very rarely a severe clinical condition for children (18). This clinical “mildness” is also witnessed by our cases, and some authors speculated on its immunological age-related factors (19). Furthermore, the initial fear of contracting COVID-19 could have driven less families to EDs for non-urgent consultations. “Stay-at-home” orders also could have resulted in more parental supervision and fewer incidents such as accidents and other injuries. In Italy, specific radio calls and TV advertisements were broadcasted in order to reduce ED direct access without previous primary care assessment/opinion. Lastly, school/nursery closure, combined with seasonal fading of other epidemics such as influenza, gave an extra contribution to the reported reduction. Quite similarly in a French study, pediatric emergency visits revealed that the COVID-19 lockdown and school closure were associated with a significant decrease of pediatric ED visits and subsequent hospital admissions with a significant reduction especially in infectious diseases (20).
Notwithstanding, minor febrile and respiratory diseases in our own experience were more frequently assessed in ED during the COVID-19 epidemic, possibly suggesting parental anxiety about this disease, primary-care reluctance to evaluate these children due to lack of personal protective equipment, and well-established hospital COVID-19 pathways within EDs (21, 22).
However, emergency/resuscitation consultations were significantly higher in March–May 2020 compared to the same trimester in 2019, possibly highlighting both longer time spent home without medical advice or clinical assessment until worsening and family unwillingness to attend either their primary care pediatrician or the ED. In addition, the hospitalization rate among children brought to EDs was significantly higher in March–May 2020 as compared to March–May 2019, thus indicating more severe clinical conditions. These assumptions are in line with a recent pediatric case series underscoring that the risk of delayed access for some emergency conditions can be much higher than that of contracting COVID-19 (23). It is of note that this may be indirectly a pandemic-related drawback which physicians and policy makers should be aware of.
As regards the length of hospital stay for inpatients and consultations for fragile children during the two considered periods, no significant differences were found, thus pinpointing that overall plan for pediatric hospital care and hospital support for children with special needs has passed unchanged through the COVID-19 epidemic.
Emergency medical transports services are often inappropriate, providing pure transportation where no immediate care is actually needed (24). Albeit EMTS involvement was activated more appropriately in March–May 2020 rather than in March–May 2019, even during the COVID-19 pandemic, we observed families misusing the ambulance as mere means of transportation in more than two-thirds of the cases.
Despite a significant reduction of deferrable consultations during March–May 2020, a trend of increased night and weekend visits for non-urgent cases was still present. This definitely questions the current Italian system which fails to provide pediatric primary care 24/7 and force families to seek for medical care directly at the ED even for minor queries.
We are aware of some limitations of our study. The size and characteristics of our work may be not representative of the whole target population especially in places where medical homes as optimal locations for children to receive care for acute, non-emergency, health concerns are available (25). Furthermore, we have no direct proofs of the underlying personal/social motivations which prompted parents to ED consultations. In addition, due to the lack of a regional centralized public health registry, the analysis of our ED databases does not allow having more clues about the final diagnosis of hospitalized patients and comparison with other reports (20). These unanswered questions may need future research.
In conclusion, our work provides a unique snapshot of the pediatric EDs demands in the era of COVID-19. Moreover, current pandemic and lockdown policies unveiled on one hand the still perduring inappropriateness of the majority of pediatric ED consultations. At the same time, thoughtful discussions on current scenario should aim to reinforce the importance of well-structured pediatric primary care, a wise and prompt community filter for disease severity, as well as a strong tackle against ED overcrowding, for the sake of all children and particularly those with special needs.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by IRB protocol N. 10 approved on 28/04/2020 regional meeting. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
FV and LZ conceived the study, drafted the manuscript, and gave final approval of the version to be published. RP, AM, SM, and MB collected and interpreted the data, revised the manuscript critically for important intellectual content, and gave final approval of the version to be published. GB analyzed the data, revised the manuscript critically for important intellectual content, and gave final approval of the version to be published. VT conceived the study, corrected the first draft of the manuscript, and revised the manuscript critically for important intellectual content. PV designed and supervised the study, revised the manuscript critically for important intellectual content, and gave final approval of the version to be published. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to Dr. Ennio Clemente for his supportive attitude toward this project.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00521/full#supplementary-material
No comments:
Post a Comment