////////////////////MRRYING OFF DTR WORRY
//////////////////JEALOUSY NBC
//////////////////WIKIP=Neurobiological theories of emotion
This article needs additional citations for verification.Please help improve this article by adding reliable references. Unsourced material may be challenged and removed. (March 2007)
Based on discoveries made through neural mapping of the limbic system, the neurobiological explanation of human emotion is that emotion is a pleasant or unpleasant mental state organized in the limbic system of the mammalian brain.
Defined as such, these emotional states are specific manifestations of non-verbally expressed feelings of agreement, amusement, anger, certainty, control, disagreement, disgust, disliking, embarrassment, fear, guilt, happiness, hate, interest, liking, love, sadness, shame, surprise, and uncertainty. If distinguished from reactive responses of reptiles, emotions would then be mammalian elaborations of general vertebrate arousal patterns, in which neurochemicals (e.g., dopamine, noradrenaline, and serotonin) step-up or step-down the brain's activity level, as visible in body movements, gestures, and postures. In mammals, primates, and human beings, feelings are displayed as emotion cues.
For example, the human emotion of love is proposed to have evolved from paleocircuits of the mammalian brain (specifically, modules of the cingulated gyrus) designed for the care, feeding, and grooming of offspring. Paleocircuits are neural platforms for bodily expression configured millions of years before the advent of cortical circuits for speech. They consist of pre-configured pathways or networks of nerve cells in the forebrain, brain stem and spinal cord. They evolved prior to the earliest mammalian ancestors, as far back as the jawless fishes, to control motor function.
Presumably, before the mammalian brain, life in the non-verbal world was automatic, preconscious, and predictable. The motor centers of reptiles react to sensory cues of vision, sound, touch, chemical, gravity, and motion with pre-set body movements and programmed postures. With the arrival of night-active mammals, circa 180 million years ago, smell replaced vision as the dominant sense, and a different way of responding arose from the olfactory sense, which is proposed to have developed into mammalian emotion and emotional memory. In the Jurassic Period, the mammalian brain invested heavily in olfaction to succeed at night as reptiles slept — one explanation for why olfactory lobes in mammalian brains are proportionally larger than in the reptiles. These odor pathways gradually formed the neural blueprint for what was later to become our limbic brain.
[edit] Brain areas related to emotion
Emotions are thought to be related to activity in brain areas that direct our attention, motivate our behavior, and determine the significance of what is going on around us. Pioneering work by Broca (1878), Papez (1937), and MacLean (1952) suggested that emotion is related to a group of structures in the center of the brain called the limbic system, which includes the hypothalamus, cingulate cortex, hippocampi, and other structures. More recent research has shown that some of these limbic structures are not as directly related to emotion as others are, while some non-limbic structures have been found to be of greater emotional relevance. The following brain structures are currently thought to be most involved in emotion:
Amygdala — The amygdalae are two small, round structures located anterior to the hippocampi near the temporal poles. The amygdalae are involved in detecting and learning what parts of our surroundings are important and have emotional significance. They are critical for the production of emotion, and may be particularly so for negative emotions, especially fear.
Prefrontal cortex — The term prefrontal cortex refers to the very front of the brain, behind the forehead and above the eyes. It appears to play a critical role in the regulation of emotion and behavior by anticipating the consequences of our actions. The prefrontal cortex may play an important role in delayed gratification by maintaining emotions over time and organizing behavior toward specific goals.
Anterior cingulate — The anterior cingulate cortex (ACC) is located in the middle of the brain, just behind the prefrontal cortex. The ACC is thought to play a central role in attention, and may be particularly important with regard to conscious, subjective emotional awareness. This region of the brain may also play an important role in the initiation of motivated behavior.
Ventral striatum — The ventral striatum is a group of subcortical structures thought to play an important role in emotion and behavior. One part of the ventral striatum called the nucleus accumbens is thought to be involved in the experience of goal-directed positive emotion. Individuals with addictions experience increased activity in this area when they encounter the object of their addiction.
Insula — The insular cortex is thought to play a critical role in the bodily experience of emotion, as it is connected to other brain structures that regulate the body’s autonomic functions (heart rate, breathing, digestion, etc.). This region also processes taste information and is thought to play an important role in experiencing the emotion of disgust.
/////////////////////NOT JEALOUSY BUT EMPATHY FOR THE MNS SUFFERING
///////////////////////MEDSCAPE=Can We Detect Signs of Autism in Very Young Children?
Posted 10/17/2007
William T. Basco, Jr., MD, FAAPAuthor Information
Social and Communication Development in Toddlers With Early and Later Diagnosis of Autism Spectrum Disorders
Landa RJ, Holman KC, Garrett-Mayer EArch Gen Psychiatry. 2007;64:853-864
Summary
Researchers conducted a prospective study at a major medical and research institution to determine how early one might detect signs of autism and autism spectrum disorders (ASDs) in children. This study followed a group of 125 children. Of these, 107 were siblings of children with ASDs and were therefore deemed at high risk for the development of autism. A smaller group of 18 children were at low risk.
On average, autism is detected after age 2, and there has been ongoing emphasis on early detection and early therapeutic intervention.
Children were enrolled in the study before 14 months of age and underwent periodic assessments of motor, language, and cognitive development along with assessment using autism screening tools. The children were evaluated a final time at between 30 and 36 months of age by blinded evaluators (in a majority of assessments). These 36-month outcomes provided the final diagnostic assignments: ASD, both early and late diagnosis; broader autism phenotype (BAP); and non-BAP, which could include impairments that were not of the BAP types.
These final diagnostic groupings were used to retrospectively analyze the children's performances on testing at 14 and 24 months.
Previous retrospective studies had suggested that children with autism and ASDs have language and other developmental deficiencies that are detectable in the first 12 to 18 months of life, but this fact had not been established in a prospective cohort. ASD was diagnosed in 30 of the children's siblings by 30 to 36 months of age, and 16 children in the current study were actually given the diagnosis of ASD at the 14-month evaluation (the early-diagnosis group).
Of the 16 children who did not receive an ASD diagnosis at 14 months but were diagnosed with ASD by the final visit, 13 exhibited at least some impairment in the domains tested at 14 months. At 14 months, the early ASD group exhibited multiple impairments, including language, joint attention, and fewer shared play experiences.
As a group, the later-diagnosis ASD group had mild impairment, but this was limited to gaze shifting. In most measures, they were not significantly different from the non-BAP group or children in the control group (those not siblings of children with ASDs). By 24 months, however, the late-diagnosis group performed significantly below the non-BAP group in 10 of 12 measures.
The authors conclude that for some children diagnosed later with autism, the diagnosis is evident at 14 months. However, there is another group of children diagnosed with autism later who, at 14 months of age, exhibit developmental performance that is not distinguishable from typically developing children.
Viewpoint
This study is fascinating for opening a window into the natural history of autism. First, the early-diagnosis group could be identified by 14 months, but the authors note that many of those children exhibited behaviors (or lack thereof) that were concerning to the parents -- this elucidated on intake questioning. This increased concern on the part of parents who already had a child with ASD likely accounts for the higher rate of ASD and BAP in these siblings of children with autism than the rates noted in other population studies. This is a highly referred and self-referred population. So the study reinforces a previous finding that parents often identify concerning behaviors during the first year of life in children later diagnosed with autism. A second point worth emphasizing, noted by the authors, is the suggestion of a continuum of ASD symptoms among siblings of children with ASD. These children with the broader autism phenotype did not qualify for ASDs by current criteria but still exhibited disruption in some skills that are deficient in children with ASDs. The bottom line is that siblings of children with ASDs are a high-risk group, and they should be followed carefully. These data suggest that they should receive formal developmental screening around both the first and second birthdays.
/////////////////SCREENING FOR AUTISM=NAME CALL OUT RESPONSE AT AGE 1 YRS
/////////////////////Pain in the Neck
Tina Simpson, MD; Jean Ivey, DSN, CRNP; Melinda B. Cooling, MS, RN, CFNP
Pediatr Nurs. 2007;33(4):342-344. ©2007 Jannetti Publications, Inc.
Posted 10/17/2007
Jacob is a 10-year-old boy who presented to an ambulatory clinic with a chief complaint of neck swelling.
History of Present Illness
Jacob had been evaluated in a local emergency room three times for swelling to the right side of the jaw. His mother stated he had a lesion near the right jaw line that looked like a "pimple" that became infected and then the swelling began. He was initially started on Keflex (Cephalexin) 250 mg three times daily for cellulitis. His condition did not improve and he was started on Augmentin (Amoxicillin/Clavulanate) 875 mg twice daily for 10 days. The anterior cervical region continued to stay enlarged and he developed adenopathy on the left anterior cervical side as well as an enlargement in the left supraclavicular area. Jacob then developed a low grade fever and the Augmentin (Amoxicillin/Clavulanate) prescription was extended to 14 days and his parents were instructed to follow up with his primary care provider. His CBC, rapid strep, and monospot were all normal, but he continued to have a low grade fever and pain when moving his neck. Jacob did not complain of sore throat, ear pain, vomiting, diarrhea, change in appetite, or malaise.
Past Medical History
His past medical history includes asthma and ADD. Immunizations are up to date.
Hobbies
Jacob has many kittens at home that he enjoys playing with. His kittens often paw at his face leading to scratches while Jacob plays with them, but he has not had any previous infections from scratches.
Current Medications
His medications included Augmentin (Amoxicillin/Clavulanate) 875 mg twice daily and Concerta 36 mg daily.
Physical Examination
Physical examination revealed a relatively healthy 10-year-old boy. Oral temperature was 98.6 F, respiration 20 breaths/minute, blood pressure 98/60, and a pulse of 88 beats/minute. The right side of the neck revealed a 10 cm x 5 cm area of cervical adenopathy that was tender to palpation, mobile, and without overlying inflammatory changes or increased local temperature. On the left side of the neck was a 7 cm x 7cm elongated adenopathy that was tender to palpation, mobile, and had increased local temperature. Additionally there was a healing 0.75 x 1 cm maculopapular lesion on the right jaw line. The remainder of the physical examination was normal.
Differentials
Cervical Lymphadenitis
In children, cervical lymphadenitis due to Mycobacterium can be common but rarely is there dissemination of the disease.
Lipomas
Cystic lesions or lipomas may also be considered but are often freely movable and come on gradually, whereas lymphadenitis appears more suddenly.
Strep
Group A strep is a common childhood disease that can present with tonsillar exudates, tender anterior lymphadenopathy, and fever. The diagnosis of Group A strep can be determined with a rapid strep test or throat culture.
Mononucleosis
Mononucleosis is a viral infection caused from the Epstein Barr Virus. Children can present with sore throats, fatigue, and lymphadenopathy. Epstein Barr titers can help differentiate past exposure or current infection with mononucleosis.
Cellulitis
Cellulitis is a bacterial infection that extends into the tissues below the outer layer of skin. If often develops where there has been an opening in the skin from a cut, bite, or burn. Cellulitis can cause tenderness, pain, redness, and edema at the site and within the surrounding area.
Discussion
History and laboratory evaluation revealed that he had Cat Scratch Disease (CSD), a self-limited infectious disease most often characterized by regional lymphadenopathy. Cat scratch fever commonly affects immunocompetent humans younger than age 21. The annual incidence overall is 3.7 per 100,000 cases per year with the highest rates in children under the age of 10 (9.3 per 100,000 per year) (Spach, Myers, & Kaplan, 2006). Normally, CSD does not lead to serious illness. There is an estimated incidence of 22,000 cases per year, with 2,000 of those requiring hospitalization due to complications. CSD occurs worldwide with seasonal increases in fall and early winter (Anderson & Edwards, 1995; Spach & Myers, 2005; Busen & Scarborough, 1997).
The most common etiologic agent is the Bartonella Henselae organism. This organism normally is transmitted from a cat through a scratch or break in the skin. Young cats or cats with fleas pose a greater threat. The animal does not act or appear ill, which makes it difficult for patients to identify CSD as a consequence of the cat or kitten (Conrad, 2001; Kravetz & Federman, 2002; Batts & Demers, 2004; Liedholm, 2002). In Jacob's case, a CBC (complete blood count), metabolic panel, Bartonella Henselae Titers, and Epstein Barr Titers were drawn. The Bartonella Henselae IGG Titer was 1:1024, supportive of the diagnosis of Cat Scratch Disease (CSD). The remainder of the laboratory data was normal.
CSD usually begins after exposure to an infected cat's saliva. A papular lesion normally develops at the site of inoculation. These lesions are often mistaken for insect bites or pimples and may be overlooked. Most often patients also present with lymphadenopathy near the site of inoculation. Involvement of the lymph system can range from enlargement of 1 to 3 lymph nodes but rarely more than 4. Many other physiological systems can be affected by CSD. These include skin, lymphatic, ocular, neurological, and visceral organs. Anorexia, malaise, headaches, abdominal discomfort, or muscle pains are common subjective findings (Busen & Scarborough, 1997; Spach & Myers, 2005; Leidholm, 2002, Lamps & Scott, 2004).
Skin
A lesion will develop at the site of inoculation 3 to 10 days later. This lesion will change from a papule to an opaque-colored fluid filled vesicle, then to a crusty maculopapular lesion, and then to a macule that may persist for months (Spach & Myers, 2005, Busen & Scarborough, 1997).
Lymphadenopathy
Regional lymphadenopathy is the hallmark sign of CSD. The lymphatic involvement is usually proximal to the inoculation site and develops 2 weeks after inoculation, and normally resolves in 1 to 4 months. Often these areas are tender with erythema of the overlying skin. Generally the lymph nodes grow to 1-5 cm, but some may enlarge to 8-10 cm. The most common lesion locations are axillary, epitroclear, cervical, supraclavicular, and submandibular areas. Generalized lymphadenopathy is rare, so another etiology may need to be considered if present (Spach & Myers, 2005; Leidholm, 2002).
Ocular
Parinaud's Oculoglandular Syndrome occurs in 2%-3% of patients and is characterized by an ocular granuloma and conjunctivitis. Swelling of the parotid gland due to preauricular and/or submandibular lymphadenopathy contributes to this disorder (Malatskey, BenDavid, Fradis, and Podoshin, 2000). This most often occurs if the cat bite or lick is near the eye or if there is self-infection from another site (Spach & Myers, 2005; Busen & Scarborough, 1997; Ormerod & Dailey, 1999). Neuro-retinitis is another ocular complication resulting in loss of vision from edema of the optic nerve associated with macular exudates. The Bartonella organism is the most common cause of this.
Neurological
Encephalopathy, myel itis, radiculitis, and cerebellar ataxia are complications involving the neurological system. Encephalopathy is the most common and patients normally present with acute confusion and disorientation. Patients with encephalopathy related to CSD, often have a normal CT scan and an abnormal electroencephalogram, and 20%-30% have mononuclear pleocytosis in the cerebrospinal fluid. Many patients will recover entirely within several weeks, but some may experience residual neurological deficits (Spach & Myers, 2005).
Visceral Organs
Patients with CSD may have liver and/or spleen involvement. Most often these patients have elevated liver function tests, fever of unknown etiology, and abnormal CT scans showing multiple, scattered hypoechoic organ defects (Spach & Myers, 2005; Kahr, Kerbl, & Gschwandtner, 2000).
In summary, the following are objective and subjective symptoms in CSD: fever, malaise, blurred vision, decreased visual acuity, and retinal changes, including hemorrhages, cotton wool spots, multiple lesions deep in the retina, or stellate macular exudates (macular star) (Spach & Myers, 2005).
Diagnosis of CSD requires careful attention to subjective and objective data. The standard diagnosis involves 3 of the 4 following: lymphadenopathy (local or regional), recent cat contact, identification of the inoculation site, positive B. henselae titers. The Bartonella Henselae Antibody is a slow growing gram negative bacteria that often exhibits titers of 1:64 or greater for B. henselae IgG titers (Spach & Myers, 2005; Busen & Scarborough, 1997; Leidholm, 2002).
There continues to be controversy regarding treatment of uncomplicated CSD. Current practice suggests that select oral antibiotics can shorten the duration of lymphadenopathy (Leid holm, 2002; Busen & Scarborough, 2002; Batts & Demers, 2004; Conrad, 2001). It has also been noted that CSD is self-limited and may resolve spontaneously in 2 to 4 months. Jacob was treated for CSD by adding azithromycin 500 mg day 1, then 250 mg days 2-5 to his current regimen of Augmentin. See Table 1 for treatment guidelines.
Follow-Up
Two weeks later, Jacob's swelling had improved. The node on the left side of the neck was decreased to 7 cm x 3 cm with mild tenderness and overlying erythema. The node on the right side of the neck was 6 cm x 4 cm with no overlying erythema and no tenderness. One week later the right side was 5 cm x 3 cm and the left side was 5 cm x 2 cm, both without tenderness or erythema.
Nursing Implications and Education
Nurses should provide education to the patient and the family regarding the medications, including side effects, how the medication works for the disease process, and appropriate dosing. In addition, careful monitoring of a CSD patient is important to prevent secondary or systemic infections as well as monitoring improvement. Patient should be monitored for unresolved lymphadenopathy, ocular or neurological disorders, and liver or spleen involvement. The patient may also need encouragement due to altered self-image due to the clinical manifestations. Assessment of the developmental stage of the child and offering support is crucial for the child and family. Frequent office visits or at times hospitalization are necessary and should be reviewed with the parents to help relieve financial or transportation stressors. Nurses should consider CSD in patients who have persistent symptoms of low grade fever, lesions, and lymphadenopathy. Early recognition can lead to decreased depression in the patient/family, better control over health care costs, continued school attendance, and less residual emotional effects on the child.
Nursing implications includes history taking about pets, discussing safety around animals, and further evaluation of presenting symptoms. Nurses can use the 2005 CDC guidelines to encourage parents or cat owners to decrease CSD risk. Many times families are concerned about the transmission among other family members. Though a cat may have scratched more than one family member, it is rare that more than one person becomes infected. It is not necessary to euthanize the cat. However, understanding the importance of judgment when handling cats is important (Busen & Scarborough, 1997).
The child's development at the time of disease is also important to consider as it may affect self-image and self-esteem. Talking with the child to describe the symptoms and recovery are essential so it is understood that most children are not left with permanent disorders from cat scratch disease. Encouraging the family to also provide support and discuss altered image at school helps the child to not feel like he or she is different.
Cats can positively influence children's and families' emotional and physical well being. Providing patient education regarding prevention of CSD (see Table 2 ) or management of the disease is essential to the well being of the child as well as enjoyment of the cat.
Table 1. Treatment of Cat Scratch Disease
Table 2. Treatment of Cat Scratch Disease
References
Anderson, B., & Edwards, K. (1995). Cat scratch disease: A mystery solved. Contemporary Pediatrics, 12(11), 17-32.
Antimicrobial Therapy, Inc. (2005). The Sanford guide to antimicrobial therapy (35th ed.). Hyde Park, VT: Gilbert, Moellering, Eliopoulos, & Sande.
Batts, S., & Demers, D. (2004). Spectrum and treatment of cat scratch disease. The Pediatric Infectious Disease Journal, 23(12), 1161-1162.
Busen, N., & Scarborough, T. (1997). Diagnosis and management of cat scratch disease in primary care. The Internet Journal of Advanced Practice Nursing, 1(2).
Conrad, D. (2001). Treatment of cat scratch disease. Current Opinion in Pediatrics,13(1), 56-59.
Kahr, A., Kerbl, R., Gschwandtner, K., et al. (2000). Visceral manifestation of cat scratch disease in children. A consequence of altered immunological state? Infection, 28(2), 116-118.
Kravetz, J., & Federman, D. (2002). Cat-associated zoonoses. Archives of Internal Medicine, 162(17), 1945-1952.
Lamps, L.W., & Scott, M.A. (2004). Cat scratch disease: Historic, clinical, and pathologic perspectives. American Journal of Clinical Pathology, 121(Suppl.), S71-80.
Leidholm, M (2002). Encountering cat scratch disease. The Nurse Practitioner, 27(2), 14, 60.
Malatskey, S., BenDavid, J., Fravis, M., & Podoshin, L. (2000). Cat scratch disease of the parotid gland: An often misdiagnosed entity. Annals of Otology, Rhinology, and Laryngology, 109(7), 679-82.
Ormerod, L.D., & Dailey, J.P. (1999). Ocular manifestations of cat scratch disease. Current Opinion Ophthalmology, 10(3), 209-216.
Spach, D.H., & Myers, S.A. (2005). Cat scratch disease. Retrieved March 14, 2007 from http://uptodateonline.com
Submitted by:Melinda B. Cooling, MS, RN, CFNP, Nurse Practitioner, OSF Medical Group, Roanoke, IL, Part-time Faculty, Bradley University, Peoria, IL
/////////////////////CHEEK BONES-SOMILY XEEKES
////////////////////1 IN 7 PRISONERS FOREIGN-11K NEARLY
////////////////Role of Rhinovirus in Hospitalized Infants With Respiratory Tract Infections in Spain Rhinovirus was detected in hospitalized infants with respiratory tract disease and was the second most common virus after RSV.
///////////////////Primary Headache and Sleep Disturbances in Adolescents Sleep disturbance is a common complaint that has long been associated with primary headaches. The aim of this study was to assess sleep patterns in teens with primary headaches using a validated sleep screening instrument.
////////////////////CME Overweight Children at Increased Risk for Asthma Hospitalization Among children who presented to the emergency department for asthma, overweight children with asthma were significantly more likely to be older and live in an impoverished area.
///////////////////CME High-Dose Ibuprofen May Slow Progression of Lung Disease in Cystic Fibrosis A study shows that this especially occurs in children, suggesting that strategies to modulate lung inflammation can be beneficial for people with cystic fibrosis.Medscape Medical News 2007
///////////////////Minority of Children With Atopic Eczema Develop Asthma Contrary to common belief, only a minority of infants and young children with atopic eczema go on to develop asthma, according to a report in the September Journal of Allergy and Clinical Immunology.Reuters Health Information 2007
//////////////////Neurologic Abnormalities Common After Periventricular Infarction Infants who survive periventricular hemorrhagic infarction commonly develop significant cognitive or motor abnormalities, according to a report in the October issue of Pediatrics.
//////////////////Sleep-Disordered Breathing Risk Seen in Young Adults With Very Low Birth Weight Very low birth weight infants have an increased risk of developing sleep-disordered breathing when they reach young adulthood, according to findings published in the October issue of Pediatrics.
///////////////////POPPY APPEAL-
/////////////////////New evidence of early human culture
Listen Now - 20102007 Download Audio - 20102007
Lumps of red ochre 164,000 years old have been found in a cave above the South African coast, east of Cape Town. Scientists suspect early humans used it to paint their bodies. There are about 57 pieces of pigment which have been scraped and ground up. The pigments don't occur naturally around the cave. There is also evidence of tools.
Erin Thomson describes the cave, and what was found. One pile of detritus, suspected as being tens of thousands of years of garbage reveals clues as to what the early people ate.
The oldest people anatomically are in Africa, and date to about 200,000 years. This evidence, from 164,000 years is the oldest evidence of people acting and behaving in ways similar to humans today.
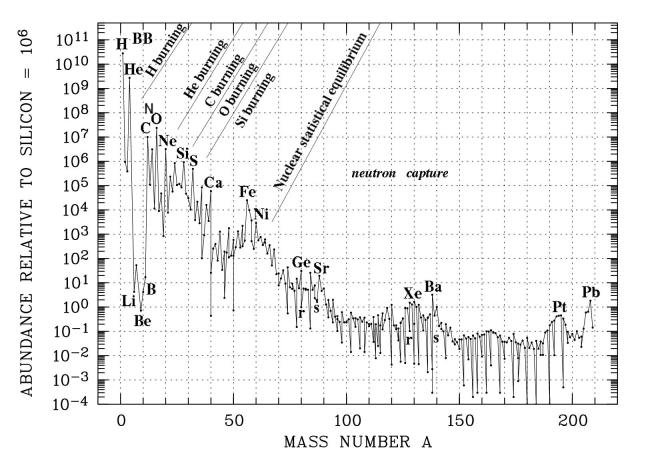
////////////////////Origin of Elements
Light elements (mainly hydrogen, helium and trace of deuterium, lithium) were generated in the first few minutes of the Big Bang, which was not able to produce more complex elements as the universe rapidly cooling off. Since then hydrogen and helium contribute by mass of respectively 70 and 28 per cent of all baryonic matter in the universe. Most of the remaining 2% of the elements up to iron and nickel are made in the interior of the stars. The resulting elements are thrust into space by booming stellar winds or when a star explodes as a supernova. Carbon, nitrogen and oxygen are the most abundant heavy elements. Oxygen is created by supernovae, while carbon is created in low-mass stars (red giants, planetary nebulae) and nitrogen is by a mixture of the above.
Figure 14-03 Element Abundance [view large
image]The rest of the heavy elements come from a poorly understood process, which requires the presence of a staggering numbers of neutrons. It is thought that such event may occur in the collision of neutron stars or from supernova explosions that form neutron stars. There are 92 elements known to occur naturally on Earth; 83 of these are stable, and the others are radioactive. More than 20 elements with atomic numbers greater than 92, have been created artificially in particle accelerators. All are extremely unstable and decay rapidly into lighter elements. The "local galactic" abundance diagram of Figure 14-03 indicates the elements from hydrogen to beryllium are generated by BB (Big Bang); heavier elements up to nickel are produced by nuclear burning inside stars; the other heavy elements come from a neutron capturing process with the neutron subsequently decays to proton. Nuclear statistical equilibrium is referred to the state in which forward and reverse nuclear reactions balance.
/////////////////OMG-WTF!!!!
///////////////////HOPE SPRINGS ETERNAL
To find out how the brain generates optimism for the future, researchers at New York University scanned the brains of 15 volunteers while they imagined possible future life events, such as "winning an award" or "the end of a romantic relationship."
The scientists discovered positive future events led to increased activity in the same brain clusters that seem to malfunction in depression—the amygdala, which helps form and store emotional memories, and the rostral anterior cingulate, which helps regulate emotional responses. The researchers also found that when volunteers had optimistic personalities, as rated by psychological exams, these brain clusters activated more.
http://www.livescience.com/health/071024-brain-optimism.html
//////////////////
You can?t say it?s in their head
Doctors still find it difficult to treat children?s abdominal pain, says Laurie Tarkan
When 12-year-old Hannah Scott began middle school last year, she was so nervous that her stomach was not just in knots, it was in serious pain. ?It would start in the morning when I?d leave the house,? said Hannah, a wisp of a girl with light brown freckles and long sandy hair. ?And when I got to school, it was really, really bad. I?d go to the nurse every other day, and be sent home.?
When the bellyaches persisted for months, Hannah?s parents took her to a paediatric gastroenterologist, who ordered tests, including x-rays, a colonoscopy and an endoscopy, to rule out serious problems. After nothing showed up, the ailment was diagnosed as irritable bowel syndrome, a gastrointestinal disorder with no organic cause and no proven treatment in children. But the doctor said there was nothing to do about it; eventually, it got so bad that her parents pulled her out of school.
An estimated 10 per cent to 20 per cent of all school-age children suffer severe recurrent abdominal pain. But many children and adolescents go for 13 to 18 months before being treated, and some are never treated at all. In some cases, untreated pain is so debilitating that they miss school, dance classes, sports activities and social events. They are at risk of falling behind academically, physically, socially and developmentally.
Experts say that organic causes like ulcers, inflammation or intestinal blockages are to blame in only a small minority of children, 5 per cent to 10 per cent. A majority suffer instead from what are called functional gastrointestinal disorders. The most common are functional abdominal pain, in which pain is the only symptom; irritable bowel syndrome, which brings on pain along with diarrhoea or constipation; and functional dyspepsia, which typically shows up as pain with nausea or a feeling of fullness.
Often, children who have recurrent abdominal pain are put through a battery of invasive tests. They are placed on restrictive diets and given large doses of acid-suppressing medications or anti-diarrhoea drugs, which may offer some relief from the symptoms, but often do nothing for pain. Some children are told that their illness is ?all in their head,? or that they are faking it.
According to gastrointestinal specialists, many doctors don?t know how to treat stomach pain in children. ?There are a lot of misconceptions that make the life of these children more difficult,? said Dr Carlo Di Lorenzo, chief of paediatric gastroenterology at the Children?s Hospital of Columbus, Ohio. ?They bounce from doctor to doctor, get more and more tests, until things get better or they find a specialist who knows how to treat them,? Di Lorenzo said. There are clear criteria for diagnosing disorders that cause recurrent abdominal pain, and for most children, the diagnosis can be made without invasive tests.
?It?s an easy diagnosis, but not for paediatricians, because they are still so lacking in their awareness that these conditions exist in children and adolescents,? said Dr Nader . Youssef, a paediatric gastroenterologist at the Goryeb Children?s Hospital in Morristown, New Jersey. New approaches to treating pain are already being used in adults, including cognitive behavioural therapy; alternative treatments like relaxation techniques and massage therapy; and antidepressants. But they have not been widely adopted for children, in part because only a handful of small studies support such use.
Gut-wrenching: Even the slightest bit of gas hurts
In recent years, however, experts have begun to understand more about the connections between the brain and the gut, a relationship that is reflected in popular expressions like ?a gut-wrenching experience? or ?having butterflies in your stomach.? The gastrointestinal tract is awash in nerve cells and neurotransmitters. About 95 per cent of the body?s neurotransmitter serotonin is in the intestinal tract. Stress, nervousness, fear and other emotions often play out their own drama in the gut. In children with abdominal pain, the intestinal tract becomes hypersensitive to stimuli, with the slightest bit of gas, for instance, sending a flood of pain signals to the brain.
The problem appears to be a mismatch in signalling between the brain and the gut, said Dr Lonnie Zeltzer, director of the paediatric pain programme at the David Geffen School of Medicine at the University of California, Los Angeles. ?If you have ongoing pain, you can develop abnormal pain pathways, so that the volume of pain signalling is being turned up and up,? Zeltzer said. What causes the hypersensitivity is not completely understood, but experts believe that it is often set off by a stomach virus or an infection. ?It?s not uncommon that a family will get viral gastroenteritis, the whole family gets better except the child,? said Zeltzer, whose book, Conquering Your Child?s Chronic Pain: A Pediatrician?s Guide for Reclaiming a Normal Childhood, will be published by HarperResource in January. ?The pain system is turned on and stays on.?
Experts do not know why some children and adolescents develop this problem and others do not. One clue may be that children with abdominal pain tend to be unusually worried and anxious. In a study published in the April issue of Pediatrics, researchers at the University of Pittsburgh interviewed children in a primary care setting and found that those with recurrent abdominal pain were 79 per cent more likely to have an anxiety disorder than those in a control group.
As an understanding of the brain-gut connection grows, however, some centres have begun to use techniques like cognitive behavioural therapy, relaxation training, massage therapy and other alternative approaches as a first line of treatment. The effectiveness of these therapies is still debated, and the number of studies examining their effectiveness in children is very small, experts say. In one study published in the August issue of The Journal of Pediatric Gastroenterology and Nutrition, 18 children ages eight through 17 who had pain for about a year were taught guided imagery and progressive relaxation.
In four to seven sessions, 89 per cent of the children reported a reduction in pain, to an average of two episodes a week, from six, said Youssef, the lead author of the study. The children had fewer missed school days, and their quality-of-life scores rose significantly. ?Our goal is to help them relax about the pain,? Youssef said. ?If you don?t worry about the pain, you don?t get pain.?
NYTNS
///////////////
Wednesday, October 24, 2007
Decoding the Human Eye
Superdense arrays of silicon electrodes will bring scientists closer to an artificial retina that approximates normal vision.
By Emily Singer
Print
E-mail
Audio » New!
Listen - Flash Listen now-->
Listen - MP3
Subscribe to podcast What is this?-->
What is this?
Powered by
Share »
Digg this
Add to del.icio.us
Add to Reddit
Add to Facebook
Slashdot It!
Add to Newsvine
Add to Connotea
Add to CiteUlike
Add to Furl
Googlize this
Add to Rojo
Add to MyWeb
Test bed: A 512-electrode array (gold circle), modeled after detectors used to capture particles in high-energy physics, is helping to decipher the neural code of the retina. The findings will aid in the design of future retinal prostheses. Credit: Alan Litke
Multimedia
•
View images of an artificial retina and it's affect on vision.
Related Articles:
•
Implantable Retinas Come Alive05/23/2006
•
Retinal Transplant Restores Vision in Mice11/08/2006
•
Next-Generation Retinal Implant02/16/2007
Other readers liked:
•
On the White Path09/25/2007
•
Landing a Spacecraft with Engines Blazing09/13/2007
•
Levitating Nanomachines08/14/2007
•
Machines Powered by Heart Muscles09/07/2007
•
E-paper with Photonic Ink09/05/2007
Artificial retinas are already in human clinical trials at the University of Southern California, where they have helped blind patients distinguish walls from doorways and even watch soccer games, albeit as blurs of motion. But approximating normal vision--and possibly enabling people to read--will require devices that can deliver electrical current with much greater control and precision. A new chip densely packed with electrodes, developed by scientists at the University of California, Santa Cruz (UCSC), is the first step in that direction.
Currently being used in research, the chip can stimulate and record from individual cells in retinal samples. The technology will provide insight into how the retina codes information and how to mimic that coding--lessons that will be crucial in developing the next generation of retinal implants. Further down the road, some version of the technology might be used to send visual information down the optic nerve.
/////////////////////
{kind=link}
No comments:
Post a Comment